- RAG rating
- n/a
- Document type
- Clinical policy
- Place
- Hertfordshire and West Essex ICB
- Output type
- Clinical Policies & Evidence-based Interventions
- Document
- Download
Injections and Radiofrequency Denervation for non-specific back pain
v1.1
This policy covers invasive treatments of non-specific low back pain4 in secondary care, excluding surgical intervention and spinal cord stimulation. It is a local policy supplement to the following national EBI Programme guidance found at https://ebi.aomrc.org.uk/:
- Injections for non-specific back pain without sciatica – EBI list 1
- Lumbar radiofrequency facet joint denervation – EBI list 2
Other related national EBI programme guidance includes:
- Low back pain imaging – EBI list 2
- Lumbar discectomy – EBI list 2
- Vertebral augmentation for painful osteoporotic vertebral fractures – EBI list 2
- Fusion surgery for mechanical axial low back pain – EBI list 2
Other related local EBI policies:
- Spinal cord stimulation
- Epidurals for radiculopathy This policy does not apply to children 16 or younger, or patients with other causes of low back pain4, such as:
- progressive neurological deficit,- cauda equina syndrome,- metastatic spinal cord compression in adults,- spinal injury,- suspected cancer- spondyloarthritis
Spinal injections
In line with the national EBI programme guidance (list 1), facet joint injections for non-specific low back pain are not routinely commissioned.
In the rare circumstance that a patient meets the guidance criteria for radiofrequency denervation, but the procedure is contraindicated (e.g. presence of pacemaker/ICD/ complex spinal anatomy/ presence of spinal metal work), and the clinician recommends facet joint injections, an individual funding request should be submitted.
Epidurals
The ICB will not routinely fund epidural injections for patients with non-specific low back pain.1
For radiculopathy, please refer to local EBI policy on Epidurals for Radiculopathy.
Medial Branch Blocks
Medial branch blocks will only be commissioned when ALL of the criteria below are met:
- The procedure is intended as a diagnostic test to localise the source of lower back pain to assess suitability for radiofrequency denervation 4.
- The patient is 16 years or older 4.
- The pain has lasted for more than 12 months duration
- The main source of pain is thought to be from structures supplied by the medial branch nerve (i.e. arising from one or more facet joints) 1,3,4
- The patient has moderate or severe levels of localised back pain (rated as 5/10 or more on a visual analogue scale, or equivalent) at the time of referral 1,3,4.
- There has been a failure of non-invasive management3 as per local pathways and Appendix 2*:
oGuided self-management, exercise programme +/- manual therapy +/- psychological therapies ORoLow intensity combined physical and psychological programme (CPPP)oComprehensive CPPP or standard pain management programme (PMP)
- The patient has been reviewed by a specialist clinician/physiotherapist trained in spinal assessment and this treatment is considered necessary to enable full participation with a rehabilitation programme.
- Where available, the patient agrees to participate in multidisciplinary rehabilitation post ablation in increase likelihood of sustained benefit3.
*It is accepted that many patients may not be able to comply with all aspects of conservative management because of pain and medial branch blocks +/- RFD may help them to engage with other conservative measures.
Repeat medial branch blocks
Repeat medial branch blocks at the same site are not routinely commissioned.
Repeat diagnostic medial branch blocks at a new site will be considered where the criteria above are met.
In the unusual circumstance that a repeat diagnostic medial branch block is thought to be necessary due to diagnostic uncertainty, an individual funding request (IFR) should be submitted. Some patients may experience a prolonged response to medial branch blockade such that further interventional treatment is no longer required. However, a prolonged initial response is not an indication for further, therapeutic, medial branch block if the pain returns.
Radiofrequency (RF) Denervation
Radiofrequency denervation will be commissioned when all of the following criteria have been met:
- All of the above diagnostic medial branch block criteria have been met.
- There has been a positive response to a diagnostic medial branch block1,3,4.
- The patient has been referred after assessment by a specialist orthopaedic or MSK service.
Imaging should not be offered as a pre-requisite for radiofrequency denervation in patients with non-specific low back pain with specific facet joint pain.1,3,4
Radiofrequency denervation will not be funded for patients who have radicular pain without low back pain. 4
Repeat Denervation
Repeat denervation at a new site will be considered where the criteria above and in the national EBI programme are met.
Repeat denervation at the same site is not routinely funded and will only be considered on an individual basis, where there has been a relapse after a clear evidence of benefit over a 16 month period, where the clinician feels that repeat is likely to be of benefit to the patient and the patient fulfils the criteria for an initial radiofrequency ablation.
Please note that the ICB will not fund any other spinal injections for patients with non-specific back pain
Appendix 1
The Back Pain Pathway Flowchart
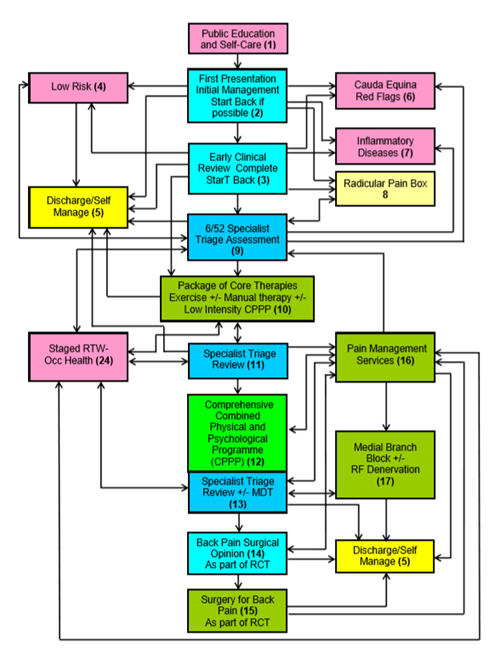
Source: extracted from the National Low Back and Radicular Pain Pathway 2017, page 14(3).
Appendix 2:
Non-invasive management
A list of non-invasive treatments for low back pain and sciatica approved by NICE and recommended by the National Low Back and Radicular Pain Pathway.
NICE approves the following non-invasive treatments for low back pain and sciatica(4):
- Guided self-management.
- Exercise (ideally group programme)
- Manual therapy (spinal manipulation, mobilisation or soft tissue techniques such as massage) for managing low back pain with or without sciatica, but only as part of a treatment package including exercise, with or without psychological therapy.
- Psychological therapies using a cognitive behavioural approach for managing low back pain with or without sciatica but only as part of a treatment package including exercise, with or without manual therapy (spinal manipulation, mobilisation or soft tissue techniques such as massage).
- Consider a combined physical and psychological programme, incorporating a cognitive behavioural approach (preferably in a group context that takes into account a person's specific needs and capabilities), for people with persistent low back pain or sciatica:
-when they have significant psychosocial obstacles to recovery (for example, avoiding normal activities based on inappropriate beliefs about their condition)or or-when previous treatments have not been effective
- Return-to-work programmes (promote and facilitate return to work or normal activities of daily living).
- Pharmacological interventions
The National Back Pain Pathway also recommends(3):
- Public Education and self-care
- GP or over the counter medication
- Self-directed exercise programme
- Self-directed relaxation techniques
- Self-directed return to normal social and occupational activities
- Core therapies:
oExerciseo+/- Manual therapyo+/- Low intensity CPP as appropriate
- Comprehensive multi-disciplinary M-CPPP or Pain Management Programme
Appendix 3
Back pain injections are commonly defined in terms of the anatomical structures targeted and whether the drug injected is being used for therapeutic or diagnostic effect.
The types of injections are:
•Therapeutic facet joint injections including: intra-articular facet joint injection, medial branch block injection
•Therapeutic epidural injections including (according to where the epidural space is accessed) which could be lumbar epidural or caudal epidural injections
•Diagnostic which helps in to determine the anatomic origin of the patient’s pain
See Table 1 for definitions
Table 1: Glossary
Clinical features suggestive of a facet joint component 3
- "Increased pain unilaterally or bilaterally on lumbar para-spinal palpation
- Increased back pain on 1 or more of the following:
-Extension (more than flexion)-Rotation-Extension/side flexion-Extension/rotation
AND
-No radicular symptoms-No sacroiliac joint pain elicited using a provocation test.”
Epidural injection -
"An epidural is an injection in the back to stop you feeling pain in part of your body.
Steroid medication can also be given as an epidural injection to treat back or leg pain caused by sciatica or a slipped (prolapsed) disc.
The epidural can be inserted at different levels of your back depending on the area of the body that requires pain relief.
There are different types of epidural depending on the approach taken: caudal, interlaminar and transforaminal.”
Facet joint -
"The spine is a column of bones arranged one on top of the other. The bones are linked at the back by joints called facet joints, on each side. The facet stabilises the spine, while also allowing movement”
Facet joint injection -
"Under x-ray control, local anaesthetic (to reduce pain in the short-term) and corticosteroid (to reduce pain and inflammation in the long-term) are injected into the targeted facet joints.”
Lower back pain -
"Lower back pain is felt in the area between the bottom of the ribcage and the top of the legs. It’s the most common type of back pain. Symptoms range from tension and stiffness to pain and soreness.
Non-specific back pain -
Non-specific low back pain is diagnosed when the pain cannot be attributed to a specific cause, although in many cases, may be related to trauma, or musculoligamentous strain.
Most people's back pain is described as non-specific, meaning it’s caused by a minor problem with the structures in the back (such as a strain) rather than anything serious.
The back is a complex area of muscles, nerves, bones and joints, and is continuously working hard to support the weight of the upper body.
It’s often unclear why lower back pain occurs, but it can sometimes be triggered by things like bending awkwardly, lifting incorrectly, standing for long periods of time, slouching when sitting, and driving for long periods. Sometimes lower back pain will come and go over time
Medial branch blocks(6) -
"Facet joint medial branch blocks is a procedure in which nerve fibres supplying the painful facet joints are blocked by local anaesthetic injections.”
Radiofrequency denervation(9) -
"Radiofrequency denervation is a specialised injection, which uses heat to alter the function of the nerves that supply the facet joints in your back. These nerves transmit the pain signals from these joints to your brain. The procedure carried out using X rays to guide the injections, in a similar way to diagnostic tests.
Radiofrequency denervation of the nerves is performed by placing special needles alongside the nerves to the facet joints, then passing an electric current through each needle. This creates heat at the needle tip, which results in a change to the structure and function of the nerve. This can lead to a reduction of pain.”
Sciatica or radiculopathy -
"Sciatica is pain caused by irritation or compression of the sciatic nerve. The sciatic nerve is the longest nerve in your body, and runs from the back of your pelvis, through your buttocks and down both legs, ending at your feet.
When something compresses or irritates the sciatic nerve, it can cause pain, numbness and a tingling sensation that travels from your lower back down your leg.
The most common cause of sciatica is a slipped (or prolapsed) disc. This occurs when one of the discs that sit between and cushion the bones in the spine is damaged and presses on nearby nerves.
Most cases will pass in a few weeks or months, although it may come and go over time. Treatments such as staying active, painkillers, and back exercises or stretches often help. In rare cases, surgery may be needed.”
Spinal cord stimulation (neuromodulation)(10) -
Spinal cord stimulation is a method that can be used to relieve pain. A small device that produces mild electrical pulses is placed inside the body by an operation. These pulses are sent to the spinal cord, causing a ‘stimulation’ effect, which changes the way a person feels pain. The feeling of pain is masked with a tingling sensation in the area of the body that normally hurts. The amount of pain relief that a person feels with spinal cord stimulation varies from person to person. As pain changes (improves or gets worse), the level of ‘stimulation’ can be adjusted. The device can also be taken out of the body at a later date if necessary.
Steroid injections (11) -
"Steroid injections, also called corticosteroid injections, are anti-inflammatory medicines used to treat a range of conditions.
Steroids are a man-made version of hormones normally produced by the adrenal glands, two small glands found above the kidneys.
When injected into a joint or muscle, steroids reduce redness and swelling (inflammation) in the nearby area. This can help relieve pain and stiffness.”
References
1. NHS England. Evidence-Based Interventions: Guidance for CCGs. (2.0):180.
2. Hutton M. Spinal Services GIRFT Programme National Specialty Report [Internet]. 2019. Available from: https://gettingitrightfirsttime.co.uk/wp-content/uploads/2019/01/spinal-surgery-report.pdf
3. NHS England. National Low Back and Radicular Pain Pathway 2017. 2017.
4. National Institute of Healthcare and Clinical Excellence. Low back pain and sciatica in over 16s: assessment and management Invasive treatments NICE Guideline NG59 [Internet]. 2016. Available from: https://www.nice.org.uk/guidance/ng59
5. NHS. Overview: Epidurals [Internet]. 2017 [cited 2006 Sep 20]. Available from: https://www.nhs.uk/conditions/epidural/
6. Guy’s and St Thomas’ NHS Foundation Trust. Facet joint medial branch blocks for the treatment of pain. 2017.
7. NHS. Overview: Back Pain [Internet]. 2017. Available from: https://www.nhs.uk/conditions/back-pain/
9. Oxford University NHS Trust. Radiofrequency Denervation of the lumbar facet joints- Information for patients. 2015.
10. NHS. Steroid injections [Internet]. 2017 [cited 2006 Sep 20]. Available from: https://www.nhs.uk/conditions/steroid-injections/