- RAG rating
- n/a
- Document type
- Clinical policy
- Place
- Hertfordshire and West Essex ICB
- Output type
- Clinical Policies & Evidence-based Interventions
- Document
- Download
Continuous Glucose Monitoring - Adults Policy
v2.0
1. Introduction
People with diabetes on insulin need to regularly monitor their blood glucose levels to judge the amount of insulin they need to inject, to keep their blood glucose within an acceptable range and reduce the risk of short- and long-term complications.
Historically, there were three main types of blood glucose monitoring: self-monitored blood glucose testing (using skin prick tests), real-time continuous glucose monitoring (rtCGM) and intermittently scanned continuous glucose monitoring (isCGM). isCGM is also sometimes known as ‘flash’. The only isCGM available in the UK (FreeStyle Libre 2) has now been upgraded to rtCGM, although it can still be used as an isCGM for patients who prefer this.
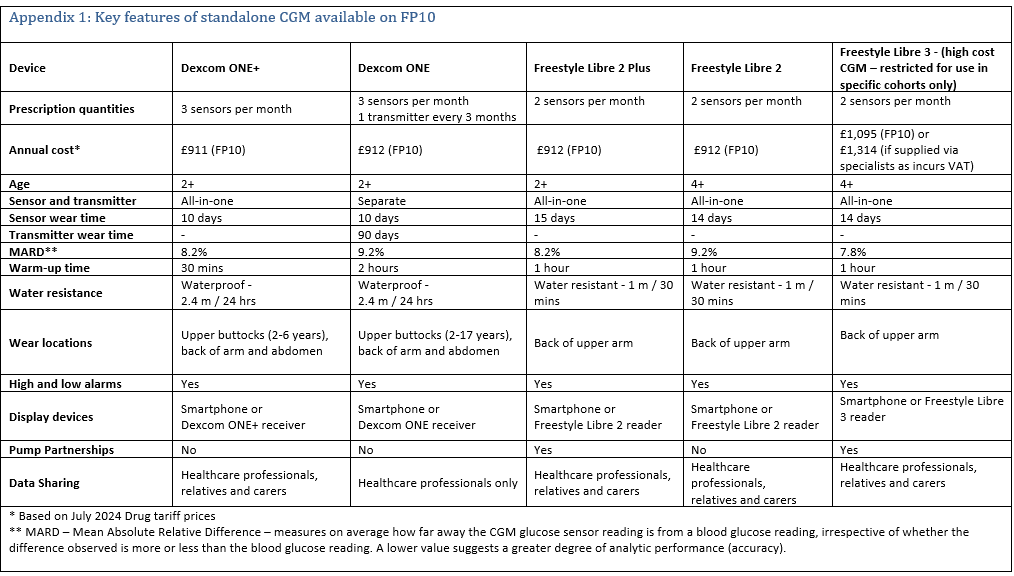
CGM devices can be divided into "low-cost” and "high-cost”. Low-cost CGM are those which cost <£1000 and are usually available to prescribe via a FP10. Formulary choices include FreeStyle Libre 2 and Dexcom ONE. These devices have sufficient functionality to meet the needs of most patients requiring CGM (see appendix 1). These models can now be upgraded to the FreeStyle Libre 2 plus and the Dexcom One + which offer even more functionality.
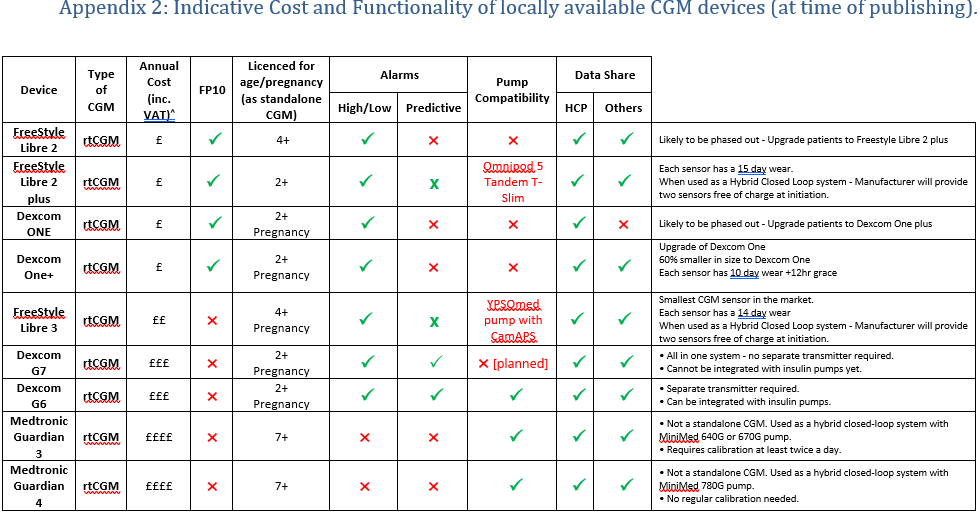
Higher cost CGM devices >£1000 on the formulary include Freestyle Libre 3, Dexcom G6 & G7, Medtronic 3 & 4. These have additional functionality which is appropriate for selected groups of patients(see appendix 2).
This policy update adds eligibility criteria for each of the different high cost CGM devices available locally, to ensure that the most cost-effective, clinically appropriate device is selected. This is essential to support any future widening of access to CGM for adults.
2. Content
Eligibility for CGM
The following cohorts are eligible for CGM:
- Adults with type
1 diabetes who are willing to commit to using CGM at least 70% of the time
and to calibrate it as needed, and who have any of the following despite
optimised use of insulin therapy and conventional blood glucose monitoring (As per the previous National Institute for Health
and Care Excellence (NICE) guidance NG17 and criteria from NHS England (NHSE)
2019 Flash guidance):
- More than 1 episode a year of severe hypoglycaemia with no obviously preventable precipitating cause.
- Impaired or complete loss of awareness of hypoglycaemia.
- Frequent (more than 2 episodes a week) asymptomatic hypoglycaemia that is causing problems with daily activities.
- Extreme fear of hypoglycaemia.
- Are clinically indicated as requiring intensive monitoring >8 times daily, as demonstrated on a meter download/review over the past 3 months
- Are unable to self-monitor due to disability
- The specialist diabetes MDT determines have occupational or psychosocial circumstances that warrant a 6-month trial of CGM
- Are living with a learning disability and it is recorded on their GP Learning Disability register
- Are pregnant (12 months in total inclusive of
post-delivery period)
- Adults with insulin
treated type 2 diabetes who are living with a learning disability and it is
recorded on their GP Learning Disability register (As per NHSE 2019 Flash guidance,)
- People with any
form of diabetes on haemodialysis and on insulin treatment who are
clinically indicated as requiring intensive monitoring >8 times daily, as
demonstrated on a meter download/review over the past 3 months (As per NHSE 2019 Flash guidance,)
- People with diabetes associated with cystic fibrosis on insulin treatment (As per NHSE 2019 Flash guidance,)
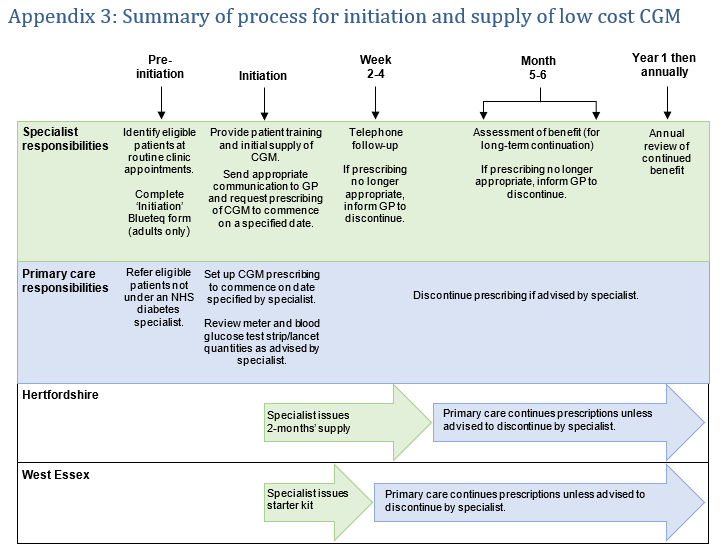
A summary on process for initiation and supply of low cost CGM has been added as appendix 3.
The Dexcom ONE and FreeStyle Libre 2 have
sufficient functionality to meet the needs of most patients requiring CGM. Both
have customisable hypoglycaemia alerts, supporting those with impaired
hypoglycaemia awareness. The Dexcom ONE is able to do repeat hypoglycaemia
alerts (e.g. if hypoglycaemia continues or reoccurs within 15 mins). The
FreeStyle Libre 2 does not do repeat hypoglycaemia alarms but, unlike the
Dexcom ONE, does enable the user to share readings with others.
Initiation of CGM is via specialist diabetes teams
only. Applications for low-cost CGM should be made by the specialist teams via
the Blueteq drug management system. The low-cost CGM devices, following
initiation by the specialists, can be prescribed via FP10 in primary care.
See Appendix 1 for a comparison document for formulary CGM devices that are available on FP10.
- Upgrading from Freestyle Libre 2 to Freestyle Libre 2 Plus and Dexcom ONE to Dexcom ONE+
All existing users of Freestyle Libre 2 and Dexcom ONE will require upgrade to Freestyle Libre 2 Plus and Dexcom ONE+, respectively. Primary care is responsible for identifying and upgrading patients using the following instructions and supporting materials.
Freestyle Libre 2 to Freestyle Libre 2 Plus
1. Change your patients' repeat prescription to the FreeStyle Libre 2 Plus sensor [PIP: 428-0194]. Quantity: 2 sensors / 30 days (1 sensor lasts 15 days).
2. Inform your patients that their prescription will be changed using the template letters circulated separately.
3. Ensure that the FreeStyle Libre 2 sensor [PIP: 416-3416] is removed from the patient’s repeat record.
Dexcom ONE to Dexcom ONE+
1. Change your patients' repeat prescription to the Dexcom ONE+ sensor [PIP: 426-8058]. Quantity: 3 sensors / 30 days (1 sensor lasts 10 days).
2. Inform your patients that their prescription will be changed using the template letters circulated separately.
3. Ensure that the Dexcom ONE sensor [PIP: 421-4722] and Dexcom ONE transmitter [PIP: 421-4730] are removed from the patient’s repeat record.
- Switching between low-cost CGM manufacturers
Patients currently receiving NHS-funded low-cost CGM who feel that an alternative manufacturer’s system is better suited to managing their diabetes should be advised to discuss this with their diabetes specialist at their next routine appointment. Specialists may switch patients to an alternative manufacturer’s device where considered suitable. Primary care clinicians should only switch the patient’s prescription to an alternative manufacturer’s device when advised to do so by the patient’s diabetes specialist.
Eligibility for high-cost CGM
Some patients will require additional functionality that is only available on high-cost CGM devices. To ensure the most cost-effective, clinically appropriate device is chosen, patients requiring a high-cost CGM device must meet both the eligibility criteria above for CGM and the criteria for the relevant high-cost CGM device.
After funding for high-cost CGM has been approved, if a patient’s circumstances change such that they are no longer eligible for a high-cost device, they should be switched to a low-cost device at the earliest opportunity, rather than at the end of the approved funding period.
The following criteria are based on the additional
functionality and cost of each device (see appendix2).
FreeStyle Libre 3
The FreeStyle Libre 3 is the least expensive of the formulary high-cost devices. It can be used as a standalone CGM with optional high/low glucose alarms and a mandatory urgent low alarm and also has data sharing capability It can be linked with a compatible insulin pump to create a hybrid closed loop system.
Criteria: One of the following must apply
- For use in children aged 4+ who have tried low cost FSL2/ FSL2 plus and Dexcom One / Dexcom One Plus, but are unable to wear the sensors due to the size and require a smaller sensor. Evidence must be provided.
- Eligible for a hybrid closed loop system and where currently using or about to start a compatible YPSOmed pump with CamAPS or currently using or about to start compatible Omnipod 5 insulin pump.
Initiation of FreeStyle Libre 3 is via specialist diabetes teams only. Applications should be made by the specialist teams via the Blueteq drug management system. An initial supply of 28 days will be supplied by the specialist teams. Primary care can be requested to take up on-going prescribing after initiation. The devices can be prescribed via FP10.
Dexcom G7
In addition to the functionality of the low-cost CGM devices and Free Style Libre 3, the Dexcom G7 has predictive alerts, which warn the wearer that they will be hypoglycaemic soon. These allow more time to act to prevent or self-treat hypoglycaemia. Like the Dexcom ONE plus, the G7 is able to do repeat hypoglycaemia alerts (e.g. if hypoglycaemia continues after the initial alert or reoccurs within 15 mins), and is also able to share readings. Dexcom G7 a cost-effective option where predictive alerts are required.
Criteria:
- Have tried low cost real-time CGM
AND
- Require predictive alerts due to at least one of the following whilst on low cost real-time CGM:
o More than 1 episode in a year of severe
hypoglycaemia (i.e. requiring 3rd party assistance) with no obviously
preventable precipitating cause
OR
o Frequent (more than 2 episodes a week) asymptomatic
hypoglycaemia that is causing problems with daily activities.
OR
o Extreme fear of hypoglycaemia that persists despite
6 months of low cost real-time CGM.
Dexcom G6
The only additional functionality of
the Dexcom G6 over the G7 is insulin pump connectivity. Used with a compatible
pump, the G6 can form a hybrid closed loop (HCL) or predictive low-glucose
suspend (PLGS) sensor-augmented pump
Criteria:
- Using an insulin pump which requires the G6 to create a hybrid closed loop (HCL) or predictive low-glucose suspend (PLGS) sensor-augmented pump.
OR
- Currently
eligible for an insulin pump and intend to start pump therapy with a compatible
pump within the next 3-6 months.
Medtronic 3 and Medtronic 4
The Medtronic 3 and 4 are not
standalone CGMs and can only be used with the Medtronic pump as part of a
low-glucose suspend (LGS) sensor-augmented pump, predictive low-glucose suspend
(PLGS) sensor-augmented pump or hybrid closed loop (HCL) system.
Criteria:
- Currently using
or about to start a compatible Medtronic pump.
Other indications for high cost CGM
Sleeping through hypoglycaemia alarms
is not an indication to switch to a higher-cost CGM. This is because manufacturer
specifications do not indicate that higher cost CGM have louder alarms.
Differences in smartphone devices may have more impact on alarm volume than the
CGM device (and its corresponding app). Patients should be supported to ensure
that their smartphone is optimally configured.
Funding for higher-cost CGM devices will be considered due to skin reactions to sensor adhesives where there is:
- Significant, documented, contact dermatitis in response to sensor adhesives that cannot be managed otherwise (e.g. through use of barrier products)
OR
- Documented
allergic reaction to sensor adhesive.
The lowest cost, clinically suitable device should be selected.
Indications outside of the criteria listed in this policy will be considered on an individual basis via the IFR route, with a review of the policy criteria if relevant additional cohorts are identified.
3. Monitoring compliance
Diabetes technology is a rapidly changing area. This policy will be closely monitored and reviewed in response to significant changes, such as the publication of the NICE TA943 on hybrid closed loops (Dec 2023)⁶ and subsequent ongoing work that is being undertaken by NHSE and NHS supply chain on products that will meet the cost-effectiveness thresholds set in NICE TA943.
Data to be monitored for all patients on CGM, and all patients eligible for CGM who have not taken it up:
- HbA1c
- Time in range
- Number of blood glucose testing strips (BGTS) used
- Hospital admissions for diabetes emergencies such as diabetic ketoacidosis (DKA) or severe hypoglycaemia.
- Episodes of severe hypoglycaemia which did not result in hospital admission.
We would expect to see an improvement in these indicators in patients on CGM. We would expect to see an improvement in HbA1c, an increase in time spent in range, and a reduction of BGTS used, hospital admissions and episodes of severe hypoglycaemia.
As per the 2022 NICE guidance regarding addressing inequalities in CGM access and uptake, other actions to be taken include:
- Monitoring who is using CGM – age, sex, ethnicity, deprivation
- Identifying groups who are eligible but have a lower uptake
- Making plans to engage with these groups to
encourage them to consider CGM.
There should also be some qualitative data monitoring to capture insights on improvements in quality of life. The data collected using the above indicators and through qualitative methods will be used to evaluate the CGM policy and to inform decisions and next steps at future policy review stages.
4. References
NHSE 2019 Flash guidance
BIBLIOGRAPHY 1. National Insitute for Health and Care
Excellence. NG18 Diabetes (type 1 and type 2) in children and young
people: diagnosis and management. 2022.
2. National Insistute for Health and Care Excellence. NG17 Type 1 diabetes in adults: diagnosis and management. 2022.
3. National Institute for Health and Care Excellence. NG28Type 2 diabetes in adults:management. 2022.
4. Digital, NHS. Quality and Outcomes Framework, 2020-21. 30 September 2021.
5. NHS Digital. National Diabetes Audit, 2020-21 Quarterly Report. 2021.
6. National Institute for Health and Care Excellence. TA943 (2023) Hybrid closed loop systems for managing blood glucose levels in type 1 diabetes
5. Associated documentation
- HWE ICB CGM Policy for adults and Paeds v1.0 FULL PAPER
- HWE ICB CGM policy supplementary document
- Prioritisation framework for HWE ICB CGM policy 2022
- Insulin Pumps v3.0 (September 2024)
- Hybrid Closed Loop Systems for Adults v1.0 (July 2024)
- Hybrid Closed Loop Systems for Children and Young People Position Statement v1.0 (July 2024)
Appendix 4: Frequently Asked Questions for low cost CGM
1. Replacing faulty sensors/transmitters or sensors that fall off before they are due to be changed
If the sensor or transmitter is suspected to be defective or if the sensor falls off before it is due to be changed, patients should contact the manufacturer as soon as possible to obtain a replacement (see contact details below). Patients will need to keep the defective sensor/transmitter and follow the instructions given by the representative. Specialists/GPs should not issue additional prescriptions to replace defective sensors/transmitters or sensors that have fallen off.
Dexcom Technical Support Line
Tel: 0800 031 5763
Details of office opening hours can be found at: https://www.dexcom.com/en-gb/contact-us-direct
Abbott Customer Careline
Tel: 0800 170 1177
Details of office opening hours can be found at: https://freestylediabetes.co.uk/contact-us
2. Quantities of blood glucose test strips/lancets
Patients who use CGM still need to take blood glucose measurements, but less often. Blood glucose monitoring is required to check the accuracy of their CGM device and as a backup when blood glucose levels are changing quickly, or the device stops working. When CGM is commenced, prescribed quantities of blood glucose test strips/lancets should reduce. Diabetes specialists initiating CGM will advise on the reduced quantity of test strips/lancets to prescribe. For further information, please see Guidance for Self-monitoring of Blood Glucose (SMBG) in patients with Diabetes Mellitus
3. Using CGM to monitor blood glucose levels for the purpose of driving
The Driver and Vehicle Licensing Agency (DVLA) has published guidance relating to the use of CGM to monitor blood glucose levels for the purpose of driving – click here to access the guidance